Κωνσταντίνος
Ορθοπαιδικός
Bougoulias.com | © 2024 | All rights reserved
Μπουγουλιάς
Χειρουργός





The latest HTML5, CSS3 and advanced JavaScript have
been used to ensure the highest compatibility.





Διευθυντής Β’ Κλινικής Σπονδυλικής Στήλης,
Νοσοκομείο Metropolitan General





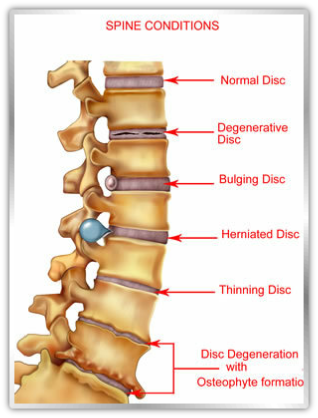
Ο μεσοσπονδύλιος δίσκος είναι το ανατομικό στοιχείο που παρεμβάλλεται μεταξύ των σπονδύλων στην σπονδυλική στήλη έχοντας σαν ρόλο την ορθή εμβιομηχανικώς κατανομή των φορτίων και την στήριξη-
Κατά την κλινική εξέταση ο ασθενής παρουσιάζει έντονο πόνο στην οσφύ (οσφυαλγία) με επέκταση στα κάτω άκρα (ισχιαλγία) ανάλογα με τον προσανατολισμό της κήλης. Ο πόνος επιτείνεται έντονα με τι κινήσεις, βήχα, πτέρνισμα. Υπάρχει μυϊκός σπασμός, ανταλγική σκολίωση, περιορισμός εύρους κίνησης της οσφυϊκής μοίρας της σπονδυλικής στήλης (όπου και στη συντριπτική πλειοψηφία εμφανίζονται οι δισκοκήλες) και πιθανώς νευρολογικά ευρήματα ανάλογα με το επίπεδο της βλάβης και την νευρική ρίζα που επηρεάζεται. Τα νευρολογικά ευρήματα συνίστανται σε έκπτωση αισθητικότητας, ισχύος και αντανακλαστικών.
Παρακλινικές εξετάσεις : ακτινογραφίες, αξονική τομογραφία, μυελογραφία, μαγνητική τομογραφία, σπινθηρογράφημα, δισκογραφία, ηλεκτρομυογράφημα, σωματοαισθητικά προκλητά δυναμικά, αιματολογικές εξετάσεις. Οι εξετάσεις αυτές ζητούνται κατά περίπτωση και με βάση την κλινική εξέταση βοηθώντας έτσι να γίνει σωστή διαφορική διάγνωση.
Θεραπεία: Η θεραπεία είναι συνήθως συντηρητική, τουλάχιστον για τα αρχικά στάδια. Αυτή συνίσταται σε ανάπαυση, θερμών συνήθως επιθεμάτων, φυσικοθεραπείας, αναλγητικών φαρμάκων τύπου παρακεταμόλης, οπιοειδών, μη στεροειδών αντιφλεγμονωδών, κορτιζόνης. Ακολουθούν ενδυνάμωση μυών, βελτίωση στάσης σώματος, απώλεια βάρους, ανάπτυξης ενός τρόπου ζωής φιλικού προς την μέση με προσοχή στον τρόπο που καθόμαστε, που αθλούμαστε, που σηκώνουμε βάρη, στο είδος του στρώματος που κοιμόμαστε κτλ. Ενδιαφέροντα αποτελέσματα παρουσιάζουν και διάφορες εναλλακτικές μέθοδοι, όπως για παράδειγμα ο βελονισμός , αλλά χρειάζεται ιδιαίτερη προσοχή στην επιλογή θεραπευτή.
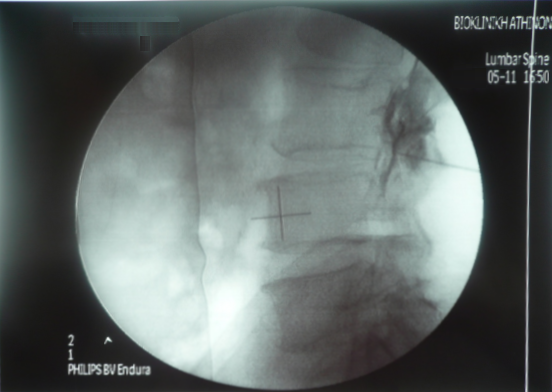
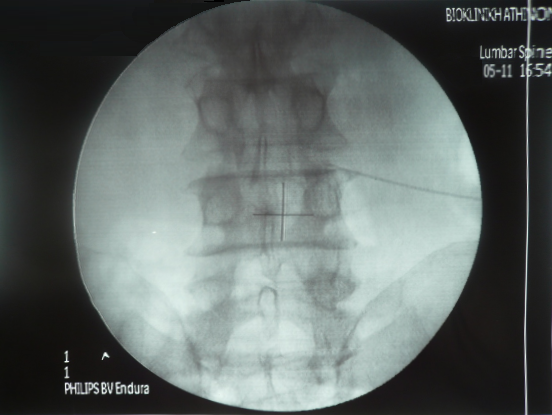
Μέθοδος μεταξύ συντηρητικής και χειρουργικής θεραπείας είναι και οι ενδοτρηματικές ενέσεις. Γίνονται στο χειρουργείο με ακτινοσκοπικό έλεγχο και τοπική αναισθησία όπου τοποθετείται με ακρίβεια η βελόνα στην είσοδο του τρήματος και επιβεβαίωση της θέσης με σκιαγραφικό. Στην συνέχεια εγχύεται κορτιζόνη και τοπικό αναισθητικό. Ο ασθενής πάει σπίτι του μετά από λίγα λεπτά και δεν χρειάζεται νοσηλεία. Βιβλιογραφικά υποστηρίζεται ότι ένα 25% των ασθενών βλέπουν μόνιμα βελτίωση και ένα 50% παροδική βελτίωση. Μεγάλη δε είναι η βοήθεια των ενέσεων αυτών και στη διαγνωστική προσέγγιση των σύμπλοκων ιδιαίτερα περιπτώσεων ώστε να επιλεγεί η κατάλληλη χειρουργική επέμβαση για τον κάθε ασθενή.

Τεράστιας δε σημασίας είναι το να αντιλαμβάνεται ο θεράπων ιατρός τα όρια όπου σταματά η συντηρητική θεραπεία και πλέον μπαίνει η ένδειξη της χειρουργικής.
Η χειρουργική θεραπεία έχει το πλεονέκτημα ότι δρα αιτιολογικά, προσπαθώντας να αναιρέσει το αίτιο του προβλήματος που είναι η κήλη του μεσοσπονδυλίου δίσκου. Αυτό πλέον γίνεται με μεθόδους ελάχιστα επεμβατικές, τη χρήση ειδικών αγκίστρων, μικροσκοπίου (μικροδισκεκτομή) όπου η βλάβη στους υγιείς ιστούς κατά την προσπέλαση είναι πολύ μικρή και οι πιθανές επιπλοκές περιορισμένες. Οφείλουμε πάντα να αναφέρουμε τις πιθανές επιπλοκές αν και σπάνιες (περίπου 1%) που είναι η φλεγμονή, τρώση μήνιγγας, βλάβη ρίζας νεύρου ή μείζωνος αγγείου ιατρογενώς, αιμάτωμα, φλεβοθρόμβωση, συνέχιση πόνου (πιθανώς εξαιτίας λανθασμένης επιλογής ασθενούς), υποτροπή κήλης. Συνήθως χρειάζεται μια μόνο ημέρα νοσηλείας και στη συνέχεια ο ασθενής ακολουθεί ένα σύντομο πρόγραμμα αποκατάστασης.
Υπάρχουν ,τέλος, περιπτώσεις όπου η χειρουργική θεραπεία είναι η πρώτη και μάλιστα άμεση επιλογή και αυτές είναι η επείγουσα νευρολογική συνδρομή με οξέα νευρολογικά ευρήματα ,όπως η πτώση άκρου ποδός όπου το πόδι παραλύει ή το σύνδρομο ιππουρίδας με παράλυση νεύρων, αναισθησία περιοχής γεννητικών οργάνων, ορθοκυστικές διαταραχές. Σε περιπτώσεις παρατεταμένης κρίσης που δεν ανταποκρίνεται στη συντηρητική αγωγή, ή πολύ συχνά επανειλημμένων κρίσεων όπου η ποιότητα ζωής του ασθενούς επηρεάζεται άμεσα, τότε συστήνουμε επίσης χειρουργική θεραπεία.


Προκαλούν όντως σύγχυση, όλοι αυτοί οι όροι, και ίσως μία φοβία στον γενικό πληθυσμό. Αυτό συμβαίνει όχι αδικαιολόγητα μιας και η χρήση κοινής ορολογίας στον ιατρικό κόσμο είναι ένα θέμα σε εξέλιξη. Στην πραγματικότητα πρόκειται περί συγγενικούς όρους που περιγράφουν την ίδια κλινική οντότητα.
Οι σκολιώσεις διακρίνονται σε λειτουργικές και οργανικές
Λειτουργικές:
1/. «Ανταλγική», όρος που χρησιμοποιείται για την κλίση της σπονδυλικής στήλης που συμβαίνει στον ασθενή υποσυνείδητα, προκειμένου να μειωθεί η πίεση σε ρίζα νεύρου όπως για παράδειγμα σε κήλη μεσοσπονδυλίου δίσκου. Έτι ο ασθενής νιώθει μια σχετική ανακούφιση, ενώ κάθε προσπάθεια να ευθειαστεί η σπονδυλική στήλη παθητικά οδηγεί σε επίταση του πόνου.
2/. Αντισταθμιστική, όπως σε ανισοσκελία, παθήσεις ισχίων κτλ. Βασικό κριτήριο αποτελεί η εξάλειψή της στην καθιστή θέση.
3/. Στατική, που οφείλεται σε ανώμαλη στάση σώματος εξαιτίας κακής νοοτροπίας, μόδας, ψυχολογικών προβλημάτων.
Οι οργανικές σκολιώσεις διακρίνονται στις παρακάτω :
1/. Συγγενής σκολίωση εξαιτίας δομικών συγγενών ανωμαλιών όπως συνοστέωση σπονδύλων, δυσπλασίες, συγγενής ημισπόνδυλος κτλ
2/. Παραλυτική, εξαιτίας συγγενών η επίκτητων παθήσεων των μυών και νεύρων και της μηχανικής ανισορροπίας που αυτό συνεπάγεται, όπως στην εγκεφαλική παράλυση, μυϊκές δυστροφίες, πολυομυελίτιδα, νευροϊνομάτωση κτλ
3/. Σκολίωση από παθήσεις του συνδετικού ιστού, όπως στο σύνδρομο Marfan, ατελής οστεογένεση κτλ
4/. Μετατραυματική σκολίωση κυρίως μετά από κατάγματα και παραμορφώσεις σπονδύλων
5/. Εκφυλιστικού τύπου σκολίωση όπου προχωρημένες εκφυλιστικές αλλοιώσεις στις δομές της σπονδυλικής στήλης οδηγούν σε σκολιωτικές παραμορφώσεις
6/. Ιδιοπαθής νεανική σκολίωση
Ο πιο συχνός τύπος, 3-
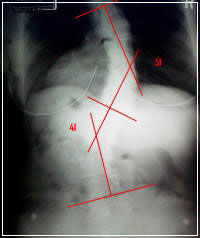 Βασικό στοιχείο στην αξιολόγηση μιας σκολίωσης είναι η κλινική εξέταση και η απεικονιστική με τη μέτρηση της γωνίας Cobb.
Βασικό στοιχείο στην αξιολόγηση μιας σκολίωσης είναι η κλινική εξέταση και η απεικονιστική με τη μέτρηση της γωνίας Cobb.
Υπάρχουν διάφορες κατατάξεις ανάλογα με την ηλικία εμφάνισης, την μοίρα της σπονδυλικής στήλης που αφορά, τα χαρακτηριστικά της παραμόρφωσης κτλ.
Η ποιο σύγχρονη κατάταξη που χρησιμοποιείται σήμερα είναι αυτή του Lenke, βοηθώντας στην εξαγωγή συμπερασμάτων για την καλύτερη δυνατή θεραπεία και την πρόγνωση.
Η θεραπεία είναι συντηρητική για μικρότερες γωνίες μέχρι 40-
Για σκολιώσεις από 15 μοίρες και πάνω συνίσταται η χρήση ειδικών κηδεμόνων 3 σημείων άσκησης πίεσης. Οι αριθμοί αυτοί δεν είναι απόλυτοι αφού άλλοι ιατροί συνιστούν τη χρήση κηδεμόνων από τις 10 μοίρες, άλλοι από τις 20 μοίρες και άλλοι συνάδελφοι υποστηρίζουν ότι η χρήση των κηδεμόνων δεν προσφέρει τίποτα (για κάθε μία από αυτές τις απόψεις υπάρχει και αντίστοιχη βιβλιογραφία να την υποστηρίζει). Η προσωπική μου πρακτική συνίσταται στη χρήση κηδεμόνων από γωνία Cobb 15 μοίρες και άνω , μέχρι την σκελετική ωρίμανση η οποία επιβεβαιώνεται κλινικά με τους δευτερογενείς χαρακτήρες του φύλου (τριχοφυϊα, φωνή, ανάπτυξη στήθους, γεννητικών οργάνων, έμμηνος ρήση) και ακτινολογικά από τη σύγκλυση των επιφυσιακών πλακών (λαγονίου, κερκίδας), οπότε και το πιο πιθανό είναι η παύση εξέλιξης της σκολίωσης.

Σκολίωση (από τη λέξη «σκολιός» που σημαίνει «στραβός») της σπονδυλικής στήλης σημαίνει παραμόρφωση της, η οποία συνίσταται σε πλάγια κλίση και στροφή των σπονδύλων και κατά συνέπεια ολόκληρης της σπονδυλικής στήλης.
Η χειρουργική θεραπεία συνίσταται για γωνίες άνω των 40-
Η χειρουργική μέθοδος που χρησιμοποιείται είναι αυτή με διαυχενικές βίδες και ράβδους μετά από οπίσθια προσπέλαση κάτω από νευροφυσιολογικό έλεγχο διεγχειρητικά. Εναλλακτικά χρησιμοποιείται πρόσθια προσπέλαση ή συνδυασμός πρόσθιας και οπίσθιας σε ένα ή δύο χρόνους.Στόχος είναι η επίτευξη σπονδυλοδεσίας με τη χρήση των υλικών και μοσχευμάτων από τον ίδιο τον ασθενή καθώς και αλλομοσχεύματα, στη νέα θέση ισορροπίας που επιτυγχάνεται διεγχειρητικά. Η κατάσταση αυτή , εφόσον επιτευχθεί τελικά οστική σπονδυλοδεσία, είναι μόνιμη και μη αναστρέψιμη. Τα υλικά δεν αφαιρούνται εκτός και αν προκαλούν κάποιο πρόβλημα.
Είναι σημαντικό να τονιστεί ότι η απόφαση σύστασης ενός κηδεμόνα σε ένα παιδί με σκολίωση είναι πολύ σοβαρή, αφού η ψυχολογική επιβάρυνση τόσο για το παιδί, όσο και για όλη την οικογένεια είναι τεράστια.
Η άσκηση μπορεί βέβαια να μην θεραπεύει, είναι όμως σημαντική για την διατήρηση της ευλυγισίας της σπονδυλικής στήλης και την ανάπτυξη του μυϊκού συστήματος.










Πιθανές επιπλοκές του χειρουργείου είναι: φλεγμονή, νευρολογική βλάβη, αγγειακή βλάβη-






Spinal pseudarthrosis; Does it really matter?
Σπονδυλική στήλη
ΕΛΑΧΙΣΤΗΣ ΠΑΡΕΜΒΑΤΙΚΟΤΗΤΑΣ ΧΕΙΡΟΥΡΓΙΚΗ ΤΗΣ ΣΠΟΝΔΥΛΙΚΗΣ ΣΤΗΛΗΣ
ΔΙΣΚΟΠΑΘΕΙΑ
ΣΚΟΛΙΩΣΗ
PSEUDARTHROSIS
ΔΙΣΚΟΠΑΘΕΙΑ, ΔΙΣΚΟΚΗΛΗ, ΚΗΛΗ ΜΕΣΟΣΠΟΝΔΥΛΙΟΥ ΔΙΣΚΟΥ, ΠΡΟΒΟΛΗ ΔΙΣΚΟΥ….ΤΙ ΠΡΑΓΜΑΤΙ ΣΗΜΑΙΝΟΥΝ ΟΛΑ ΑΥΤΑ;

REVIEW ARTICLE
K. Bougoulias
Introduction:
One of the main worries of a spinal surgeon that perform spinal fusions is failure of the attempt to get the fusion completed, ending in non union or pseudarthrosis. Master techniques and various substances such as autografts, alografts, demineralised bone matrix, BMPs and several instrumentation devices have been developed to increase the chances of solid fusion. The aim is stability and as a result of that, better clinical outcome, but, do these things go necessarily together with the solid fusion?
The answer to this question will come from a literature review and that is the main aim of this review article.
Literature review:
Pseudarthrosis is defined as lack of continuity in the fusion mass at any point from the cephalad to caudal transverse process on one or both sides (Vacaro et al 1997). The radiographic way to confirm a pseudarthrosis is through plain radiographs seeing disturbance of trabecular continuity. Dynamic films and tomograms can be even better to prove breaks in the bony continuity and localised motion in the fusion mass. Bone scan is a very good indicator but the most accurate way in the diagnosis of pseudarthrosis is computed tomography. Clinical signs are sharply localised pain over the fusion area and progression of the deformity or disease. Overall, surgical exploration is the absolute way to confirm that a fusion is completely solid.
Risk factors of pseudarthrosisare are older age (>55 years), osteoporosis, number of segments fused( maybe because of volume-
Herkowitz et al (1991) compared results in patients who undergone single level laminectomy for spinal stenosis and anterolisthesis with patients who had laminectomy and spinal non instrumented fusion for the same reason. This was a prospective study of 50 patients who presented with degenerative lumbar spondylolisthesis with complains of leg pain related to spinal stenosis isolated to single level L4-
Although, it was not the main aim of the study, it was shown that a solid fusion is not necessary for a satisfactory outcome. A fibrous fusion may decrease the degree of translation and therefore result in pain relief in low back pain and leg pain.
39 patients with the diagnosis of pseudarthrosis were compared to a matched group of patients with identical diagnosis and operative treatment but with solid fusion (DePalma et al, 1968). The authors found that there was not marked difference in terms of back pain, sciatica, return to work and level of activity between the two groups.
Another study about degenerative lumbar spondylolisthesis and spinal stenosis was done, comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation (Fischgrund et al, 1997). Studying this article, we can come in very interesting conclusions about the clinical significance of pseudarthrosis. 68 patients with the above pathology and treatment were evaluated. Arthrodesis was proved radiologicaly by Xrays and considered successful if it was shown a continuity in the fusion mass between the cephalad and caudal transverse processes. Pseudarthrosis was determined from the lack of the above radiologic sign or if lateral flexion-
A very interesting study was done by Kornblum et al (2004). It was a prospective, randomised study on 47 patients with single level symptomatic spinal stenosis and spondylolisthesis who underwent posterior lumbar decompression with bilateral posterolateral arthrodesis.
It was found that the clinical outcome was good to excellent in 86% of the patients with solid fusion compared with 56% of patients with pseudarthrosis in regards to back pain and lower limb function. There was no statistically significant difference discovered between the two groups with respect to preoperative symptomatology, age , sex, levels fused, smoking, diabetes or peripheral vascular disease. There were no postoperative infections. These factors are mentioned because, although may influence the fusion rate, they are not mentioned in most of the older studies. However , even in this study by Kornblum et al , the number of patients is too small to come in conclusions about the above factors. It was admitted by the authors that in short review, good to excellent results had been reported in patients despite the pseudarthrosis but these results had not been maintained over time. They demonstrated that approximately 85% of patients with solid fusion would maintain a satisfactory result even after 5 years..
Similar results were reported by Deguchi et al,( 1998). They did a retrospective study of 83 patients who had posterolateral fusion for isthmic spondylolisthesis. Radiological fusion and clinical satisfaction rates were 78% and 71% respectively, showing a strong positive correlation between radiological fusion and clinical success rates.
Kim et al (2005) published a study about pseudarthrosis in primary fusions for adult idiopathic scoliosis and reported a positive correlation between higher fusion rates and better clinical outcomes. Patients with pseudarthrosis had poorer scores in the SRS-
Most of the above literature is referred to the lumbar spine, but , are things different in other parts of the spine?
Tribus et al (1999), published a study about cervical spine symptomatic pseudarthrosis following anterior cervical discectomy and fusion attempt. They procceded to revision of the fusions through anterior cervical plating. 81% of the 16 patients achieved solid fusion but only 69% of them had good to excellent results. This result comes into agreement with Newman (1993) who reported that 70% of patients with established cervical spine pseudarthrosis were symptomatic enough and required revision surgery. From the ones who had successful revision ending in fusion , 69% converted to good or excellent results. The same idea of clinical improvement after successful revision surgery following pseudarthrosis supported by other authors as well (Brodsky et al, 1992; Farey et al, 1990).
The above studies used plain Xrays for radiological assessment of the spinal fusions. Plain radiographs are clearly not the perfect method for analysis of spinal fusion (Christensen 2004). The development of a more detailed radiographic system is necessary, such as CT scan, despite the obvious difficulties for study purposes ( cost, radiation etc). Up to the most recent studies, plain Xrays are still the golden standard. Lenke et al (1992) categorized Xray fusion patterns in four categories:
1/. Definitely solid fusion (solid big trabeculated bilateral fusion masses)
2/. Possibly solid fusion (unilateral large fusion mass with contralateral small fusion mass)
3/. Probably not solid (small thin fusion masses bilaterally)
4/. Definitely not solid ( graft resorption bilaterally or fusion mass with obvious bilateral pseudarthrosis)
Discussion:
It is a fact that there is nothing in the literature that is referred specifically to the clinical significance of that common condition of pseudarthrosis. It was necessary to gather informations about that issue from articles which were done for different aims but, indirectly, they were giving informations about pseudarthrosis. There is only one exception; this very recent article from Kim et al (2005) which was done specifically about the pseudarthrosis, but it was referred to correction of adult idiopathic scoliosis and involved fusion attempts in multiple spinal levels ending in higher pseudarthrosis rates.
The older literature gives the impression that there is not marked difference in the clinical outcome between solid fusion and pseudarthrosis which was in a way reassuring of fusion operative surgery. The explanation that was proposed was that a fibrous union that takes place provides satisfactory stability and results in satisfactory outcome. Also, questions can be raised about the initial indications of surgery and whether or not fusion was necessary from the first place, so, the clinical outcome would be independent to the success of the fusion. In a situation of non union and good clinical outcome, it has to be one of the two, either the fibrous tissue is enough or the indication from the beginning was wrong. The other alternative is that the Xray evaluation is not accurate and we can have non unions which are not clearly demonstrated and pass as unions or the opposite, solid unions that are not clearly demonstrated radiographicaly and are considered as pseudarthrosis. Clinical evaluation is not also very accurate because back and leg pain can be caused by other reasons and local tenderness under pressure exist in patients with confirmed solid fusion as well.
On the contrary, the latest literature support the idea that there is statistically significant difference in the outcome of solid fusion and pseudarhtrosis. That is supported by the fact that revision surgery and achievement of solid fusion in patients with symptomatic pseudarthrosis, improved their clinical status (Brodsky et al, 1992).It has also been shown that the degree of spondylolisthesis following a pseudarthrosis is higher (Deguchi et al, 1998; Fischgrund et al,1997; Herkowitz et al, 1991).
Our impression is that the satisfactory outcome starts from the good patient selection and correct indication. We also think that it really matters if the fusion attempt would be successful or not and it is worthy to make any effort to achieve solid arthrodesis (surgical technique, additional substances etc); However, confirmed pseudarthrosis does not necessarily require new surgery and only a chronic symptomatic pseudarthrosis merits revision surgery.
Bibliography:
Brodsky AE, Khalil MA, Sassard WR, Newman BP; “Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair” Spine 1992; 17: 1137-
Christensen FB; “Lumbar spinal fusion: Outcome in relation to surgical method choice of imlant and postoperative rehabilitation” Acta Orthop Scand Suppl. 2004; 75(313): 1-
Deguchi M, Rapoff AJ, Zdeblick TA; “Posterolateral fusion for isthmic spondylolisthesis in adults: analysis of fusion rate and clinical results” J Spine Disord. 11(6): 459-
DePalma A, Rothman R; “The Nature of Pseudarthrosis”, Clin. Orthop. 59:113, 1968
Farey ID, McAfee PC, Davis RF, Long DM; “Pseudarthrosis of the cervical spine after anterior arthrodesis: Treatment by posterior nerve root decompression, stabilization and arthrodesis” J Bone Joint Surg (Am) 1990; 72: 1171-
Fischgrund J, Mackay M, Herkowitz H, Brower R, Montgomery D, Kurz L; “1997 Volvo Award Winner in Clinical Studies: Degenerative Lumbar Spondylolisthesis With Spinal Stenosis: A Prospective, Randomized Study Comparing Decompressive Lminectomy and Arthrodesis With and Without Spinal Instrumentation” Spine 22(24);2807-
Herkowitz H, Kurz L; “Degenerative Lumbar Spondylolisthesis With Spinal Stenosis: A Prospective Study Comparing Decompression With Decompression and Intertransverse Process Arthrodesis” J Bone Joint Surg Am. 1991; 73:802
Kim Y, Bridwell K, Lenke L, Rinella A, Edward C; “Pseudarthrosis in Primary fusions for Adult Idiopathic Scoliosis: Incidence, Risk Factors and Outcome Analysis” Spine 30(4); 468-
Kornblum M, Fischgrund J, Herkowitz H, Abraham D, Berkower D, Ditkoff J; „Degenerative Lumbar Spondylolisthesis With Spinal Stenosis: A Prospective Long-
Lenke LG, Bridwell KH, Bullis D, Betz RR, Baldus C, Schoenecker P; “Results of in situ fusion for isthmic spondylolisthesis” J Spinal Disord. 5(4); 433-
Newman M; “The outcome of pseudarthrosis after cervical anterior fusion” Spine 1993; 18: 2380-
Tribus CB, Corteen DP, Zdeblick TA; “The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine” Spine 24(9); 860-
Vaccaro A, Garfin S; “Degenerative Lumbar Spondylolisthesis With Spinal Stenosis, A Prospective Study Comparing Decompression With Decompression and Intertransverse Process Arthrodesis: A Critical Analysis” Spine 22(4); 368-











σπονδυλικη στηλη, σπονδυλική στήλη, δισκοπαθεια, δισκοκηλη, κηλη μεσοσπονδυλιου δισκου, προβολη δισκου, τι πραγματι σημαινουν ολα αυτα, δισκοπάθεια, δισκοκήλη, κήλη μεσοσπονδυλίου δίσκου, προβολή δίσκου, τι πράγματι σημαίνουν όλα αυτά, σκολιωση σπονδυλικης στηλης, σκολίωση σπονδυλικής στήλης, σχολιωση σπονδυλικης στηλης, σχολίωση σπονδυλικής στήλης, ψευδαρθρωση, ψευδάρθρωση, ψευδαρθρωσις, ψευδάρθρωσις